Background Information
Definitions
Spontaneous pneumothorax: presence of air in the pleural space, between the visceral and parietal pleura, that occurs in the absence of trauma or medical intervention.
Tension pneumothorax is a life-threatening condition characterised by intrapleural pressure rises sufficiently to cause significant hemodynamic compromise, typically due to a one-way valve effect that traps air in the pleural space.
Causes and Risk Factors
Causes of pneumothorax are classically divided into the following: [Ref1][Ref2]
| Type | Causes |
|---|---|
| Spontaneous | Spontaneous pneumothorax occurs spontaneously, without any preceding trauma / medical intervention.
Spontaneous pneumothorax can be sub-classified into:
|
| Traumatic |
|
| Iatrogenic |
|
Complication
Acute Complications
- Progression into tension pneumothorax
- Persistent air leak / failure of lung re-expansion
- Respiratory failure
- Obstructive shock (mostly seen in tension pneumothorax, where the mediastinal shift compresses the great veins and reduces preload)
Chronic Complications
- Recurrence is common (>50% recurrence risk after 1st episode, higher in the presence of underlying lung disease)
- Persistent air leak and failure of lung re-expansion
Diagnosis
Clinical Features
Symptoms
Sudden onset of:
- Pleuritic chest pain
- Dyspnoea
Signs
Typical respiratory examination findings:
| Examination aspect | Typical findings |
|---|---|
| Chest expansion | ↓ on the affected side (due to pain) |
| Percussion | Hyper-resonant over the affected area |
| Tactile fremitus | ↓ on the affected side |
| Auscultation | Reduced / absent breath sound over the affected area |
Additional findings that suggest tension pneumothorax:
- Haemodynamic instability
- Trachea deviation (away from the affected side) and distended neck veins
- Typical signs but have low sensitivity
- Absence does NOT exclude diagnosis
Investigation and Diagnosis
1st line: chest X-ray (PA and lateral views)
- Typical finding is a visible pleural line with lung markers only visible up to this line, no longer visible beyond the pleural line
- Ultrasound is increasingly used to identify pneumothorax (e.g. in eFAST)
2nd line (if chest X-ray is equivocal): CT chest
Tension pneumothorax should be a clinical diagnosis. Do not delay interventions to obtain imaging if tension pneumothorax is suspected clinically.
Management
Tension Pneumothorax
Immediate management: chest decompression with needle decompression Insertion of a 14-/16-gauge needle until the pleura is punctured, indicated by a pop and/or sudden reduction in resistance. Note this is different from needle aspiration.
- Tension pneumothorax secondary to trauma → 4th/5th intercostal space in the mid-axillary line
- Non-trauma related → either 2nd intercostal space in the mid-clavicular line OR 4th/5th intercostal space in the mid-axillary line
Definitive management: chest drain insertion should always follow initial chest decompression
Tension pneumothorax should be a clinical diagnosis. Do not delay interventions to obtain imaging if tension pneumothorax is suspected.
Regarding the site of needle decompression, it is very unlikely for exam questions to make one to choose between 2nd intercostal space in the mid-clavicular line, and 4th/5th intercostal space in the mid-axillary line.
They are both technically correct (latest ATLS recommends 4th/5th intercostal space in trauma-related tension pneumothorax due to easier access and higher procedural success rate), and it also depends on the underlying cause of tension pneumothorax (trauma vs non-trauma).
Spontaneous Pneumothorax
Simplified Management Flowchart
Disclaimer: This simplified flowchart omits details regarding whether it is safe to intervene Safe to intervene generally defined as:
for visual clarity. Refer to the full management algorithm below for complete guidance.
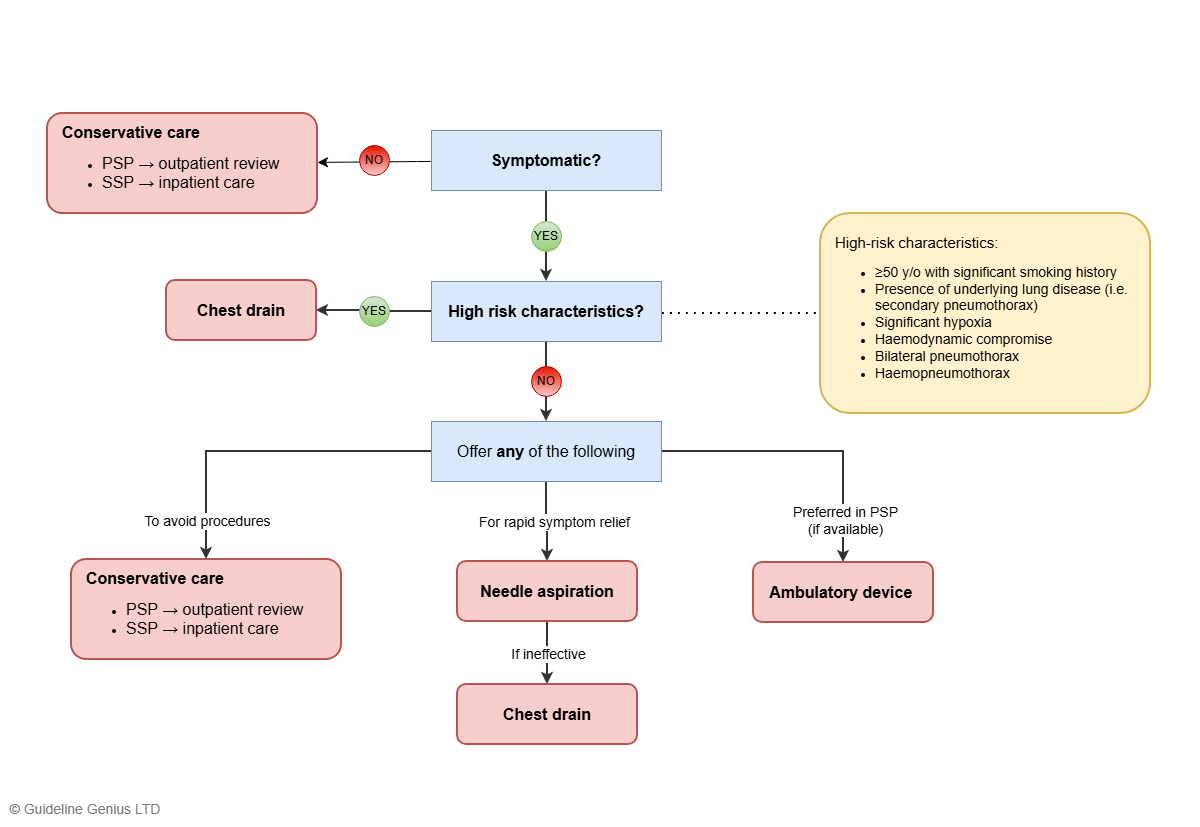
Full Management Algorithm
Symptomatic Pneumothorax
Assess for any of the following high-risk characteristics to determine subsequent steps:
| Patient factors |
|
| Pneumothorax factors |
|
High-Risk Characteristics Present
Determine whether it is safe to intervene Safe to intervene generally defined as:
- Yes → chest drain insertion
- No → perform CT scan and reassess (chest drain insertion is safe under CT guidance irrespective of size)
Subsequent care following chest drain insertion
- Admit as inpatient with daily review
- Remove chest drain when resolved
- Discharge and review as outpatient in 2-4 weeks
No High-Risk Characteristics
Determine whether it is safe to intervene Safe to intervene generally defined as:
- Yes → offer a choice of conservative management or interventional options, depending on the goal outlined below
- No → only offer conservative management
Management options:
| Goal | Recommended management | Description |
|---|---|---|
| Patient wishes to avoid procedures | Conservative management |
|
| Rapid symptomatic relief | Needle aspiration The standard site for needle aspiration is 2nd intercostal space in the mid-clavicular line. It involves inserting a 14-16 guage cannula, under local anaesthesia into the pleural space and attaching it to a syringe (often via a three-way tap, to withdraw trapped air). Air is aspirated until resistance is felt or the patient’s symptoms improve, indicating lung re-expansion. The needle should be inserted just above the rib to avoid the neurovascular bundle. |
|
| If locally available (preferred in PSP)Primary spontaneous pneumothorax | Ambulatory device |
|
Asymptomatic Or Minimal Symptoms
Always offer conservative care regardless of pneumothorax size
- If PSPPrimary spontaneous pneumothorax (PSP) → discharge and review as outpatient every 2-4 days
- If SSPSecondary spontaneous pneumothorax (SSP) → admit as inpatient for a minimum of 24 hours with supplemental oxygen
Expected pneumothorax resolution time:
- 1cm pneumothorax → ~10 days
- 2cm pneumothorax → after 2-3 weeks
Post-discharge Advice
- Return to emergency department immediately if further breathlessness develops
- Advice smoking cessation to reduce risk of recurrence
- Patients can only fly 7 days after full resolution confirmed on CXR
- Patients should be advised to permanently avoid diving, unless a definitive preventive strategy has been performed (e.g., surgical pleurectomy)
References
ATLS® Advanced Trauma Life Support® Student Course Manual 10th Edition. 2018 American College of Surgeons.
NICE Guidelines on Tension Pneumothorax
BTS Spontaneous Pneumothorax Guidelines (2023)