Background Information
Classification
Physiological neonatal jaundice:
- >24 hours after birth
- Always unconjugated (indirect) hyperbilirubinaemia
- Typical duration
- <14 days in term babies (born ≥37 weeks)
- <21 days in preterm babies (born <37 weeks)
Pathological neonatal jaundice:
- Onset <24 hours after birth
- Can be either unconjugated (indirect) or conjugated (direct) hyperbilirubinaemia
- Typically causes prolonged neonatal jaundice
Prolonged neonatal jaundice:
- Duration
- >14 days in term babies (born ≥37 weeks)
- >21 days in preterm babies (born <37 weeks)
Causes (to be added)
Complications
Note that only unconjugated bilirubin can cross the blood-brain barrier:
- Severe unconjugated hyperbilirubinaemia can result in:
- Acute bilirubin encephalopathy and/or
- Chronic bilirubin encephalopathy (aka kernicterus)
Conjugated bilirubin cannot cross the blood-brain barrier:
- Negligible neurotoxicity
- Main complications result from the underlying cause
Diagnosis Guidelines
Bilirubin Measurement
Timing
- Suspected/obvious jaundice < 24 hrs of life → measure within 2 hours
- Suspected/obvious jaundice ≥ 24 hrs of life → measure within 6 hours
Method of Measurement
There are 2 ways to measure bilirubin levels:
| Approach | Description | Indications |
|---|---|---|
| Serum bilirubin | Gold standard method (most accurate):
|
|
| Transcutaneous bilirubin | Screening method:
|
|
Serum bilirubin (NOT transcutaneous bilirubin), is used to guide management of neonatal jaundice.
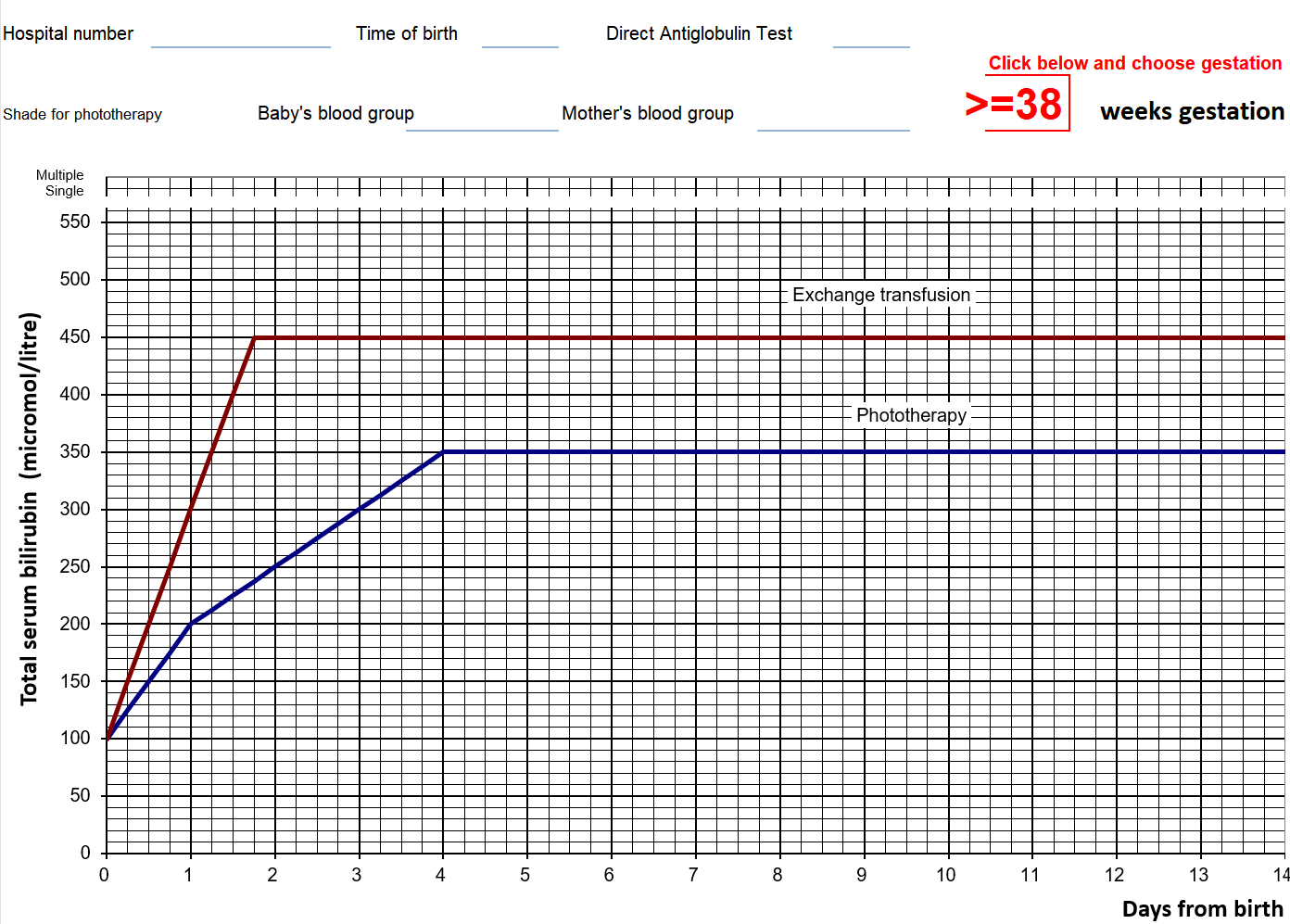
Treatment graphs for phototherapy/exchange transfusion plot serum bilirubin against post-natal age (for 3 gestational age bands).
Investigating Underlying Cause (to be added)
Management Guidelines
Management
Reassure that breastfeeding, nappy‑changing and cuddles can usually continue
If on/above treatment line → offer corresponding treatment accordingly (i.e. phototherapy or exchange transfusion)
- If the bilirubin level is within 50 mmol/L below the phototherapy threshold → repeat bilirubin measurement
- Otherwise, no routine repeat measurement is required
Note that serum bilirubin level is used to guide management (NOT transcutaneous bilirubin).
Example of a treatment threshold graph (exam questions always provide this table, and the thresholds depend on gestational age):
Phototherapy
Phototherapy should be given using an artificial light source (not natural sunlight)
Educate parents about phototherapy:
- Eye protection required
- Increased risk of dehydration
- Short breaks for feeding, nappy changes, and cuddling are encouraged
- Bronze baby syndrome
Bronze baby syndrome is a rare complication seen in neonates undergoing phototherapy.
It is characterized by a diffuse, grayish-brown discoloration of the skin, serum, and sometimes urine, which develops during phototherapy and is distinct from jaundice.
The pathogenesis is not fully understood, but it is hypothesized to involve the accumulation of photodegradation products of bilirubin.
is a rare but benign condition
Monitoring
Monitoring during phototherapy:
- Repeat 4-6 hours after initiating phototherapy
- Repeat every 6-12 hours when the serum bilirubin level is stable / falling
Monitoring after phototherapy:
- Repeat 12-18 hours after stopping phototherapy (to detect potential rebound)
Stopping Phototherapy
Only stop phototherapy when:
- Serum bilirubin level is at least 50 mmol/L below the phototherapy threshold
Intensified Phototherapy
Phototherapy can be intensified by adding another light source or increasing the irradiance of the initial light source
Consider if:
- Serum bilirubin level is rising rapidly (>8.5 mmol/L per hour), or
- Poor response (bilirubin continues to rise/does not fall within 6 hours of initiating), or
- Serum bilirubin is within 50 mmol/L below the threshold for exchange transfusion after 72 hours since birth
IV immunoglobulin can be used as an adjunct to intensified phototherapy. Indication:
- Rhesus or ABO haemolysis (i.e HDNHaemolytic disease of the newborn ), AND
- Bilirubin rising at a rate of >8.5 micromol/L/hr
Exchange Transfusion
Exchange transfusion should be performed in an intensive care bed
- Use a double volume exchange transfusion
Double volume exchange transfusion refers to the process by which a volume of blood equal to approximately twice the infant’s total blood volume is sequentially removed and replaced with donor blood or reconstituted blood products.
- Do not stop any ongoing phototherapy